
What is Cycle Threshold (Ct), Why it Matters, and Why Positive Cases Do Not Correlate to Future Deaths

Originally published at Non-Network News.
Understanding Cycle Threshold (Ct) will help you better interpret and analyze what the rise in positive Covid cases means. Most major news outlets have been constantly reporting on the dramatic increase in positive results with built-in implications. Dishonest media, pundits, and politicians would have gullible masses believe that a rise in the number of cases is indicative of the pandemic advancing, a "dark winter" to come. They use phrases like "super-spreader event" to imply that the event in question will cause mass infections, and thus deaths. But, does a spike in cases mean death is coming?
SUMMARY: The short answer is we don't know without more info. The spike in positive results means little without clinical context, i.e. what were the Ct values, were the patients symptomatic or asymptomatic, how long did the patient carry the virus, or was the virus active or inactive. Additionally, a rise in cases is directly proportional to the number of tests given, so the more tests that are given, the more cases will be detected. To fully understand the state of the pandemic using number of cases, a "viral culture is required as a reference to test for infectivity" for all PCR positive results to determine if the patient is actually contagious. Using PCR positive results and number of cases to determine public policy (in an election year) is irresponsible when number of cases does not correlate to future deaths.
In an article titled, PCR positives: what do they mean?, The Department of Physics and Technology at The Artic University of Norway (UiT) concluded that:
Conclusion: symptoms and signs of Covid19 are necessary to support the claim that the subject is or can be infectious. But calling PCR positives “cases” does not specify whether the persons have carried the virus for long or whether it is “active”. This could lead to the finding of many “cases” as a function of the number of PCR tests conducted. For example, if 20% of a population are PCR positive, the number of PCR positives will depend on the size of the sample. This means that the more PCR test are carried out the larger the fraction of the population that is confirmed but this might not speak of changes in the population. That is, it is possible that the population was infected already long before deciding to test and PCR positives would therefore not speak of “an advancing pandemic.”

Figure 2. The shaded area shows that up to X days, i.e. 10 days approximately after infection, the virus is infectious. But then the virus is still present many days after. This could result in PCR positive but it does not mean that the virous is virulent or infectious, rather it means that residues and “non active” viral RNA is still detectable by PCR. [source]
Further, not only did UiT's review of evidence submitted by The Oxford University Center for Evidence-Based Science (CEBM) confirm that an increase in PCR positives directly correlates to the number of tests given and that positive results don't mean the pandemic is advancing, they also determined that PCR positives do not mean excess deaths in the future:
The R2 number however, and Figures 4, 7, 8 and 9 (provided below) , show that PCR positives do not correlate to excess deaths in the future. The implication is that PCR positives lack predictive power in terms of telling whether people will die in the future. A possible explanation could be that the PCR positives simply measure the number of PCR tests taken on a given day, i.e. they might be somewhat proportional to the number of PCR taken on a given day, and positives might or might not be “infectious” positives. Ultimately, this means PCR positives cannot be used to tell if the pandemic is advancing if for that we understand that deaths are to increase or decrease. This agrees with the interpretation of CEBM above.
To understand what these two statements mean, we need to first understand what is a PCR positive and what does R2 mean?
According to the FDA and CDC, there are two-types of Covid-19 tests: diagnostic (or viral) tests which show if a patient currently has an active coronavirus infection or antibody tests which "look for antibodies that are made by your immune system in response to a threat, such as a specific virus." The FDA adds:
Antibodies can take several days or weeks to develop after you have an infection and may stay in your blood for several weeks or more after recovery. Because of this, antibody tests should not be used to diagnose an active coronavirus infection. At this time researchers do not know if the presence of antibodies means that you are immune to the coronavirus in the future.
Currently there are two types of diagnostic tests -- molecular tests, such as RT-PCR tests, that detect the virus’s genetic material, and antigen tests that detect specific proteins on the surface of the virus. The CDC reports PCR Testing results to track cases and says, "The 'gold standard' for clinical diagnostic detection of SARS-CoV-2 remains RT-PCR."

Wikipedia defines R2:
In statistics, the coefficient of determination, denoted R2 or r2 and pronounced 'R squared,' is the proportion of the variance in the dependent variable that is predictable from the independent variable(s). It is a statistic used in the context of statistical models whose main purpose is either the prediction of future outcomes or the testing of hypotheses, on the basis of other related information.
In other words, R2 is a statistic that can help us determine if a rise in number of cases (independent variable) means a rise in future deaths (dependant variable). It doesn't.
So, what does all this mean?
It means our governments are using the rise in the number of PCR positives to influence and determine policy when "the science" suggests that using PCR positives to determine how the pandemic is advancing is impossible without clinical context.
What's worse, is these RT-PCR tests are hyper sensitive because they record positive results for samples that have a cycle threshold of 35 to 40.
Cycle threshold (Ct or Cq) is the number of times (cycles) a sample has to be amplified before the virus can be detected. A low Ct value indicates a strong viral load because it took less cycles to detect the virus. A high Ct value indicates a weak viral load because the sample had to be amplified many more cycles to detect it.

Positive case results don't include the Ct values for each test, so "a single Ct value in the absence of clinical context cannot be relied upon for decision making about a person’s infectivity" according to Public Health England, an agency of The Department of Health and Social Care in England. We can easily check all the FDA approved RT-PCR manufactures here and sort by "Attributes" to isolate all of the companies producing approved RT-PCR tests in the United States. Instruction For Use (IFU) documents like these two below show approved tests indicating positive result can have Ct up to 39 and 40. Case numbers being reported by dishonest news as a way to imply we're headed towards a "dark winter," do not distinguish between strong and week positives, or contagious or not contagious. Without analyzing the positive results with regards to the Ct and viral load, answering the question, "When is Covid, Covid?" becomes impossible.


Dr. Fauci, talking in his own words, tells about why high Ct's above 35 will lead to more positive results for viral detection but the virus is not really contagious at those levels:
What is now, sort of, evolving into a bit of a standard [is] that if you get a cycle threshold of 35 or more, that the chances of it being replication-competent are minuscule. So that if somebody, and you know we do, we have patients and it’s very frustrating for the patients as well as for the physicians, somebody comes in and they repeat their PCR and it’s like 37 cycle threshold. But, you never, you almost never can culture virus from a 37 threshold cycle. So, I think if somebody does come in with 37, 38, even 36, you got to say, "you know, it’s just dead nucleotides period." - Dr. Fauci on This Week in Virology ep. 641 on 07/16/20
The Center for Evidence-Based Science continues:
Our impression is that most data for all countries is in agreement with our interpretation, namely, PCR positives do not correlate to deaths in the future and are therefore meaningless, on their own, to interpret the spread of the virus in terms of potential deaths......This could result in PCR positive but it does not mean that the virous is virulent or infectious, rather it means that residues and 'non active' viral RNA is still detectable by PCR....As shown the PCR positives do not correlate to excess deaths in the future and therefore lack predictive power.
Now that you have a better understanding of what Ct is and why it's so important to be able to understand what positive results actually mean, and you found out that some of the tests we're using have a Ct of up to 40, and you found out that cases doesn't mean future deaths, we can only speculate as to why and how, in an election year, could virtually everyone get it so wrong? But, slowly people are getting better information.
This NY Times article from August 29th pointed out:
One solution would be to adjust the cycle threshold used now to decide that a patient is infected. Most tests set the limit at 40, a few at 37. This means that you are positive for the coronavirus if the test process required up to 40 cycles, or 37, to detect the virus.
Tests with thresholds so high may detect not just live virus but also genetic fragments, leftovers from infection that pose no particular risk — akin to finding a hair in a room long after a person has left, Dr. Mina said.
Any test with a cycle threshold above 35 is too sensitive, agreed Juliet Morrison, a virologist at the University of California, Riverside. 'I’m shocked that people would think that 40 could represent a positive,' she said.
A more reasonable cutoff would be 30 to 35, she added. Dr. Mina said he would set the figure at 30, or even less. Those changes would mean the amount of genetic material in a patient’s sample would have to be 100-fold to 1,000-fold that of the current standard for the test to return a positive result — at least, one worth acting on...
...The C.D.C.’s own calculations suggest that it is extremely difficult to detect any live virus in a sample above a threshold of 33 cycles. Officials at some state labs said the C.D.C. had not asked them to note threshold values or to share them with contact-tracing organizations.
I had to go back to the internet archive (long load time) to confirm this since the CDC has since removed the reference showing a median Ct value of 33. But I did find Figure 5 at the very bottom of the page pretty interesting.

Figure 5. CDC unpublished data showing median Ct values and their 95% confidence intervals among specimens from which replication-competent virus was recovered and not recovered according to the Ct value for the amplification target (N1, N2, or N3) in the CDC RT-PCR assay. RNP = human RNase P, a positive control for the presence of adequate human sample. Red dots indicate specimens with inconclusive RT-PCR amplification according to their corresponding Ct values and culture results.
A friend with more insight into these things mentioned, PCR with a Ct of 30 produces 1 billion replications whereas a PCR with a Ct of 40 produces 1 trillion replications. This means that there is stark contrast between results with different Ct values and without more information, it's impossible to know what a rise in cases actually means. "The science" does show that a rise in cases does not mean a rise in future excess deaths.
Anyone who says or implies otherwise is wrong, and their motives and/or credibility should be questioned.
Referenced Figures

Figure 4. PCR positives in Spain (Top in green) versus deaths labelled as Covid19 deaths (Bottom brown) from march to the 14th of September in Spain according to the Ministry of health. [data source] (FYI, I got a page not secure warning with the data source link for Spanish data.)

Figure 7. Normalized excess deaths in Spain (blue) against PCR positives (black). [source]
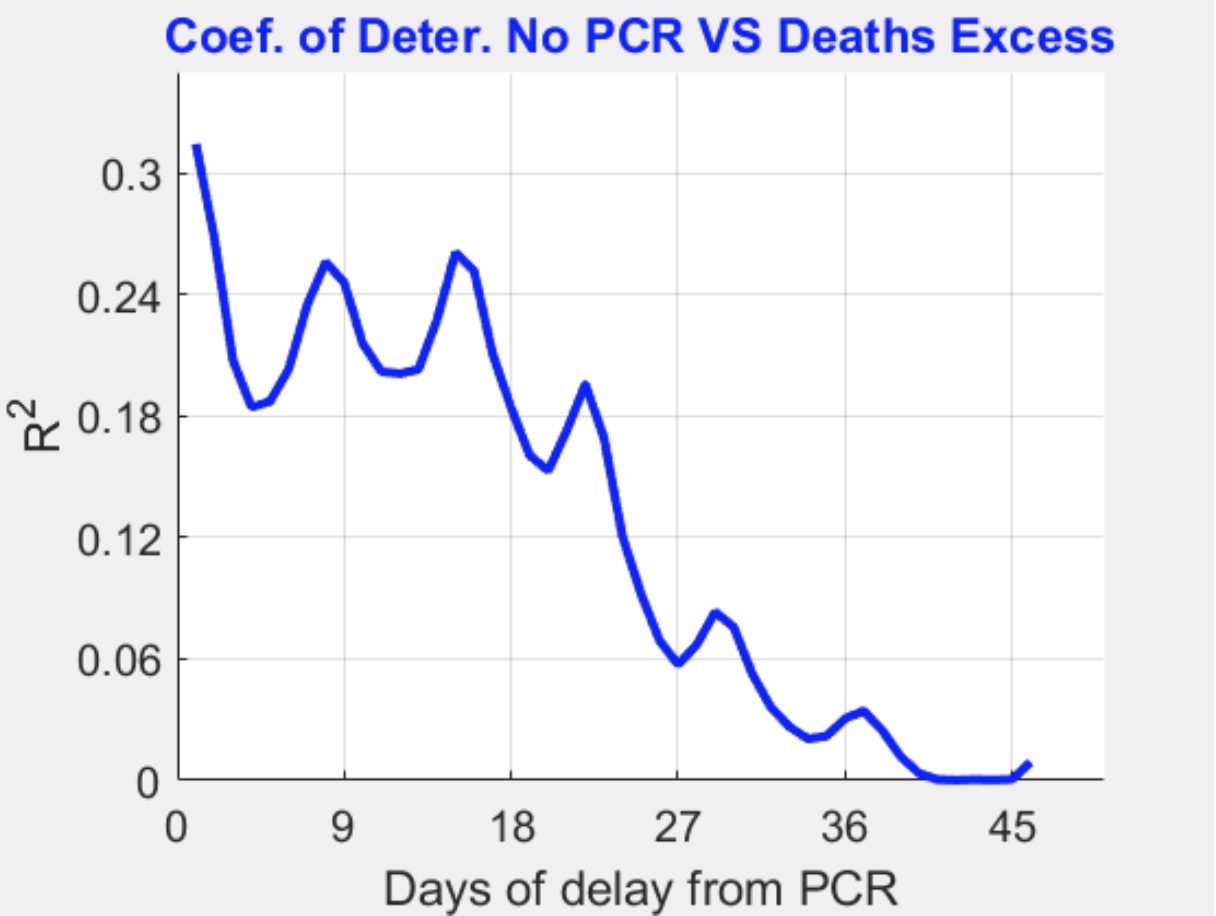
Figure 8. The x axis stands for the days of delay from the number of PCR positive recorded to the number of excess deaths. For example, if the X PCR positives were recorded today, 27 days of delay would mean that X is mapped to the excess deaths 27 days after the recording of the PCR positives. The y axis gives the coefficient of determination R2 as a function of days of delay. The highest values correspond to the proportionality between excess deaths “today” and “PCR positives today” implying that PCR tests lack any predictive power by being redundant at most.). [source]

Figure 9. Scatter plot showing PCR positives versus excess deaths from may to the end of August. The coefficient of determination R2 is 0.3 and is highest when plotting the PCR positives recorded on the same day that excess deaths are recorded. The implication is that PCR positives have no “predictive power” since in this way they cannot predict if excess deaths will follow from PCR positives. As shown in Figure 8, the more delay we give to PCR in relation to excess deaths, the lower R2. A delay of at least a few days to weeks would be meaningful since governments could “expect” what is to come in the future on the basis of the number of PCR positive cases recorded. As shown the PCR positives do not correlate to excess deaths in the future and therefore lack predictive power. [source]